|
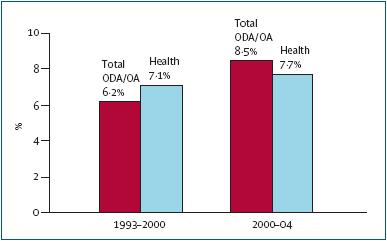
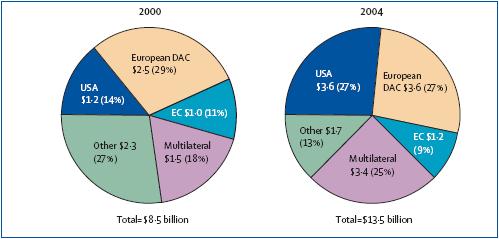
With global health likely to be high on the agenda of this year’s G8 Summit, starting today in St Petersburg, Russia, it is worth taking stock of international assistance funding trends and prospects. High-level attention to global health has risen markedly over the past two decades, particularly since 2000. One concrete measure of the priority placed on health by donors is the level of funding provided for the developing world. Previous analyses have shown that funding has been on the rise. Our analysis of data from 2000 to 2004 found a continuation of this trend, with donor funding for global health approaching US$14 billion in 2004—in part good news, as donors seem to have heeded the global health call. Still, funding for health falls far short of global need, as estimated, in part, by the WHO Commission on Macroeconomics and Health, which found that donors would need to provide an additional $22 billion a year by 2007 and $31 billion a year by 2015 to help finance the scaling-up of essential interventions, health-system development, and research and development devoted to the diseases of the poor. In addition, investments in health seem to be uneven, raising cautionary notes about the global community’s ability to meet, let alone sustain, fi nancing needs over time. Our observations are based on preliminary analysis of donor health funding in the form of official development assistance (ODA) and official aid (OA) commitments as reported to the Creditor Reporting System (CRS) of the Organisation for Economic Cooperation and Development (OECD) Development Assistance Committee, defined for these purposes to include: health; population programmes; and water and sanitation. Despite limitations in the CRS data, as acknowledged by OECD and others, the data provide an important indicator of trends over time. Between 2000 and 2004, gross new commitments by donors for total ODA/OA increased from a nominal $61·3 billion to over $104 billion. Some of the increase was offset by inflation and an exchange-rate devaluation of the US dollar against most currencies. A considerable portion went to Iraq and Afghanistan and to debt relief. Within these totals, reported funding for health rose from $8·5 billion to $13·5 billion, although its growth rate lagged behind that of total funding (59% vs 70%) and other major sectors. Health represented about the same share of total ODA/OA in each period (14% in 2000 and 13% in 2004). In constant dollars, health funding grew at an average annual rate of 7·7%, roughly the same rate of growth as in 1993–2000 (7·1%). One change, however, is that although health growth per year slightly outpaced total ODA/OA growth in the earlier period, the opposite was true between 2000 and 2004 (figure 1).
Within health, funding for HIV/AIDS and sexually transmitted diseases contributed most to sector growth, rising faster than other key health subsectors and reaching 21% of health funding in 2004, up from 8% in 2000. Other key subsectors that drove growth were infectious disease control, basic health care and, to a lesser extent, medical research. All others accounted for less than 5% of health ODA/OA in 2004, and drove little growth (1% or less). Funding for basic health infrastructure, medical education and training, and development of health personnel, the three subsectors that most directly support capacity-building, amounted to only 2% of funding in 2004 (3% in 2000). Funding for basic health infrastructure actually declined. The continued rise in donor funding for global health is a welcome sign given strains on governmental budgets and competing international demands. At the same time, gaps between resource needs and funding persist and threaten to widen, and the eff ects of infl ation and currency devaluation mean that the real rate of growth in health funding has not picked up pace in recent years. Even funding for HIV/AIDS, which grew faster than other key health subsectors, continues to fall far short of estimated need.8,9 Perhaps of more concern, however, are the imbalanced gains and gaps in investment we saw in training and infrastructure, raising critical questions about the long-term eff ectiveness of current donor eff orts and those of aff ected countries, and sobering in light of the severe global defi cit in the health-care workforce highlighted in the 2006 World Health Report.10 These are all formidable challenges that will hopefully be confronted in St Petersburg and beyond. Jennifer Kates, J Stephen Morrison, Eric Lief Kaiser Family Foundation, Washington, DC 20005, USA (JK); and Center for Strategic and International Studies, Washington, DC, USA (JSM, EL)We declare that we have no conflict of interest.
www.thelancet.com Vol 368 July 15, 2006 |